


Orthopos XG 3D cone beam imaging

Cone beam imaging, while a relatively new technology to dentistry, has already radically transformed the way that we as dentists can gather information, with the result being an ability to diagnose and treatment plan in a manner that previously could not even be imagined. The transformation from interpreting two-dimensional information to diagnosing from 3-D imaging, which allows for visualisation of all structures in any given field, is a quantum leap ... and one that has forever altered the way we must practice dentistry.
I am by no means implying that 3-D images are required for all patients, but rather am stating that I strongly believe that there are cases where two dimensions are simply not enough, and the addition of the third dimension - when applicable - becomes the only means of providing an accurate diagnosis. 3-D cone beam imaging has raised the bar and redefined the standard of care for many areas of dental practice.
Cone Beam Volumetric Tomography is a diagnostic imaging technology that uses radiation in a manner similar to conventional radiographic imaging, with the difference being that cone beam images are converted into a three-dimensional view that can then be manipulated by sophisticated computer software for a wide variety of applications, including implant, endodontic, orthodontic,periodontic , orthognathic ,TMJ, and diagnostic purposes.
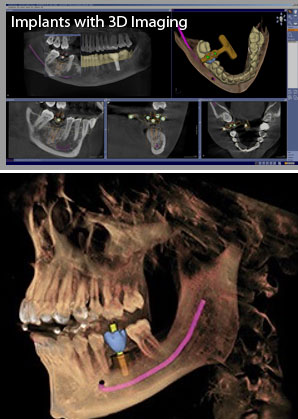 In implant treatment planning, we have come to hold the strong opinion that the standard of care today in implant dentistry is to recommend 3-D imaging for implants for nearly every patient, and because of this it would be poor practice to do implants without using 3-D imaging.
In implant treatment planning, we have come to hold the strong opinion that the standard of care today in implant dentistry is to recommend 3-D imaging for implants for nearly every patient, and because of this it would be poor practice to do implants without using 3-D imaging.
To my surprise, however, I found that 3-D imaging became indispensable in a wide range of dental diagnosis and treatment planning, to the point that there are many cases today where we cannot even imagine understanding how to best help a patient without the use of the third dimension. I found applications in endodontics with visualising fractured roots, periapical pathology, and accessory canals; in treatment planning for the extraction of third molars in proximity to the mandibular nerve; in diagnosing pathology of all types; in understanding the cause of previously undiagnosed pain; in visualising sinus pathology; in understanding the etiology of temporomandibular joint dysfunctions; and in diagnosing the true extent of periodontal pathology and disease in localized areas.
I am well aware of the orthodontic applications of 3-D imaging regarding impacted , accessory and malpositioned teeth.
For dentistry, "winning and losing" is not primarily a financial consideration. Winning and losing ultimately deals with the quality of care that we provide our patients, and doing all within our means to assure the best outcome for every procedure we perform. The third dimension in dentistry raises the odds for consistent success.